
Field Brief: Naloxone in Cardiac Arrest — When the Dogma Catches Up to the Street
- John Gomez

- 1 day ago
- 8 min read
The American Heart Association put a sentence in the 2023 Focused Update that closed a debate the field was still having.
Administration of naloxone in cases with cardiac arrest has not been shown to improve patient outcomes.

For three years, that line sat in protocols, in CE slide decks, and in code-team huddles as the authoritative answer. It was the sentence used to talk down the new medic who pushed naloxone after the first round of epi on a young arrest. It was the sentence used to explain why standing orders in a half-dozen states deliberately excluded naloxone from the OHCA algorithm.
In May 2026, Wang et al. published the largest cohort study to date on this question in JAMA Network Open. The numbers are uncomfortable for the sentence. The mechanism story is uncomfortable for the sentence. The accompanying editorial — written by two of the most respected resuscitation researchers in the world — is especially uncomfortable for the sentence.
This is not a call to start pushing naloxone before epi. It is a call to stop treating the 2023 AHA language as a closed question, because the data say it is not closed.
What Wang 2026 Actually Found Re: Naloxone & Cardiac Arrest
The Wang et al. cohort drew from the California Resuscitation Outcomes Consortium — 8,195 adult out-of-hospital cardiac arrests across three Northern California counties between 2015 and 2023. The exposure was prehospital naloxone administration by EMS during the resuscitation. The outcomes were ROSC, survival to hospital discharge, and survival with good neurologic function (Cerebral Performance Category 1–2).
Patients who received naloxone had:
An 8.1% rate of survival to hospital discharge versus 4.4% in the no-naloxone group
A 2.8% adjusted absolute increase in survival to discharge after multivariable adjustment for age, sex, witnessed arrest, bystander CPR, initial rhythm, and EMS response time
A 3.3% adjusted absolute increase in ROSC
A 3.2% adjusted absolute increase in good neurologic outcome at discharge
Translated to numbers a medic remembers under fluorescent station lights: the number needed to treat with naloxone was 9 for ROSC and 26 for survival to hospital discharge.
For context — twenty-six.
That is roughly the NNT cited in the original PARAMEDIC2 epinephrine-vs-placebo trial for ROSC, and a better NNT than the survival-to-discharge benefit epinephrine produced in that trial.
These are observational data. The randomized trial — NaCRA, NCT06251609 — is enrolling out of UCSF and will not report for at least another year. But Wang 2026 does not stand alone. The Quinn et al. cohort published in JAMA Network Open in 2024 — 3,811 California arrests across 2021–2022 — found a similar signal: an 11.8% absolute increase in ROSC and a 3.9% absolute increase in survival to discharge. Two cohorts. Same direction. Same general magnitude. Larger than the 2023 AHA language anticipated.
The Surprise Buried in the Subgroup Analysis
Here is the finding that made the editorial board sit up.
In both the 2024 and 2026 cohorts, naloxone was associated with improved outcomes not only in cardiac arrests with a clear opioid mechanism, but also in arrests where no opioid involvement was suspected.
If naloxone’s only value in arrest were opioid receptor antagonism, the benefit should disappear in non-opioid-mechanism arrests. It did not.
Two explanations are on the table.
The first explanation is that opioid involvement is being undercounted. Fentanyl analogues are now contaminating stimulant supplies, sedative supplies, and counterfeit prescription drugs. The "clean" cardiac-mechanism arrest in a 38-year-old with no opioid history is, in 2026, not as clean as the data field labels suggest. Some fraction of "non-opioid" arrests in the cohort were almost certainly occult opioid arrests. The NACARDI decision instrument was built precisely because that signal is now too loud to ignore in dispatch and field clinical pictures.
The second explanation is that naloxone has effects beyond μ-receptor antagonism. This is not new science. A 1985 Annals of Emergency Medicine case series suggested benefit in post-countershock electromechanical dissociation. Animal models from the 1990s and 2000s show naloxone augments sympathetic tone, triggers endogenous catecholamine release, and stabilizes sodium and potassium channels — Class I and Class III antiarrhythmic behavior that resembles, in mechanism if not magnitude, the drugs we already give in refractory VF/VT.
Reasonable people are arguing about which explanation matters more. Reasonable people are not, anymore, arguing that there is no signal.
What the Evidence Does Not Say
The Field Editor’s job here is to be honest about what these data are and are not.
They are not a randomized trial. Patients who received naloxone in these cohorts were, in expectation, patients whose providers suspected opioid involvement. Even after adjustment for witnessed arrest, age, initial rhythm, and bystander CPR, there is residual confounding the cohort design cannot scrub. The benefit may be smaller than the unadjusted numbers suggest. It may also be larger. We will know when NaCRA reports.
They do not establish a dose, a route, or a timing. The Wang cohort reflects what California paramedics actually did — naloxone given somewhere in the resuscitation, dose and route at provider discretion. We cannot tell you from this data whether 0.4 mg IV after the first epi is the right answer, or 2 mg IV with the first epi is the right answer, or 4 mg intranasal en route is the right answer. The trial we want has not been done.
They do not displace high-quality CPR, early defibrillation, or airway management. Anyone reading this who walks out of a station tomorrow with "naloxone is the new epi" written on their glove is reading the wrong article. Compressions. Defibrillation. Ventilation. Then the drug algorithm. Naloxone, where indicated, fits into the algorithm — it does not replace any rung.

What the evidence does say is that the 2023 AHA sentence is now harder to defend than it was when it was written. The Grunau and Rea editorial that ran alongside Wang 2026 used careful language, but the substance is clear: the field should expect this guidance to evolve.
Should You Push It? A Decision Engine
Four scenarios. No participation trophies. The dose, the timing, and the not-now answers are all part of the same call. Work through it before the next code does.
Dosing — and the 2-mg Bomb Problem
If you are going to give naloxone in arrest, give it like the drug it is.
The 2-mg IV "bomb" that became standard in many urban EMS systems in the 2010s — pushed to wake the patient, end the call, and get back in service — is not the right dose for the patient in cardiac arrest. That patient is not breathing because they have no perfusing rhythm, not because their brainstem is opioid-suppressed. The dose-response for naloxone in arrest is not the dose-response for naloxone in respiratory depression.
The 2 mg bomb in arrest is also the dose that makes the post-ROSC patient — when you get one — a vomiting, sympathetically-flooded, hypertensive, sometimes-seizing problem in the back of the truck on the way to the ED. Acute opioid withdrawal in a patient who just regained a pulse is a manageable problem. It is not a free problem.
Most of the operational protocols that have started incorporating naloxone in arrest follow one of two patterns:
Sequenced with epi: 2 mg IV/IO with or immediately after the first dose of epinephrine. Single dose only. No redose during the code.
Conservative titration: 0.4 mg IV/IO after the first epi. No redose during the code.
Either is defensible. Pick one and write it down. Do not leave it to individual provider discretion in the back of a working code at 0300. The cleanest version of this is a one-line addition to the standing OHCA algorithm: "Suspected opioid involvement or unwitnessed arrest in patient under 60: consider naloxone 2 mg IV/IO after first epinephrine." That is a sentence a medical director can write into a protocol on Tuesday and audit on Friday.
The Mechanism Argument, Briefly
Because somebody on shift is going to ask: yes, the non-opioid signal in the cohort data is biologically plausible.
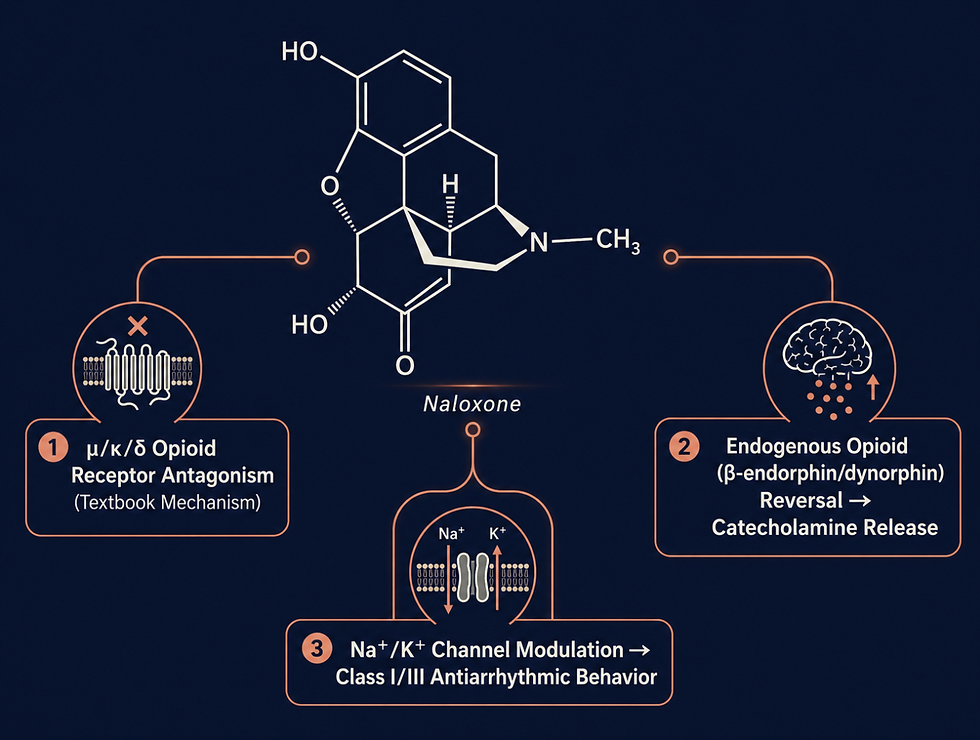
Naloxone is a competitive μ-, κ-, and δ-opioid receptor antagonist. That is the part everyone learned in medic school. The part the textbook spent half a paragraph on is that naloxone — at the doses we actually give — also blocks endogenous opioid peptides, including β-endorphin and dynorphin. Those peptides surge during severe cardiovascular stress. They contribute to the myocardial depression and vasodilation seen in shock and arrest. Naloxone, by blocking them, releases that brake.
The Class I/III antiarrhythmic story is older and weirder. Naloxone exhibits sodium- and potassium-channel-blocking behavior at concentrations achievable with standard dosing. The clinical magnitude is unclear. But the molecular behavior is documented.
None of this is a green light to give naloxone instead of amiodarone in refractory VF. It is a green light to stop treating the non-opioid benefit signal as a statistical artifact.
What This Means for Your Next Code
Until NaCRA reports — at minimum 2027, more likely 2028 — here is what working clinicians and medical directors should do.
For the medic on the truck: if your standing orders permit naloxone in arrest, give it in the patient who fits the clinical picture (suspected opioid involvement, drug paraphernalia on scene, signs of recent use, age and demographics consistent with overdose risk, witnessed apnea preceding arrest). Give it as a single 2 mg IV/IO dose after the first epinephrine. Do not redose within the code. Do not delay compressions, defibrillation, or airway to give it. Document the rationale.
For the medic whose standing orders are silent: bring this conversation to your medical director with the Wang and Quinn citations. Standing-order silence in 2026 is harder to defend than it was in 2024.
For the medical director: the language of the 2023 Focused Update was reasonable for the evidence base of 2023. The evidence base of 2026 supports — at minimum — adding a "consider naloxone" line to the OHCA algorithm for suspected opioid involvement. The systems that wait for the next AHA cycle are betting against two cohorts and a plausible mechanism.
For the QA/QI lead: track the metric. If you are adding naloxone to the algorithm, track ROSC rate, survival to discharge, and post-ROSC complication rate (withdrawal-mediated vomiting, agitation requiring sedation) by quarter. The dataset that will move the next AHA update is the dataset agencies build now.
For the educator: this is the case study to bring to the next CE block. Two cohort studies, an editorial, a pending RCT, and a guideline sentence under pressure — students should be able to articulate where the evidence is strong, where it is uncertain, and what a defensible protocol looks like in the gap.
The Closing Note
The 2023 AHA Focused Update was written by people doing the best they could with the evidence in front of them. That is what guidelines are. They are also, by design, conservative. They lag the literature by years, and they lag the field by longer.
The Wang 2026 cohort is the moment the guidance starts to fall behind. It is not the moment to publish the next algorithm — that is what NaCRA is for. But it is the moment to stop using the 2023 sentence as a conversation-ender. The conversation is open again. The data say so. The mechanism says so. The editorial in the same issue of the same journal says so.
The medics who have been giving naloxone in arrest, quietly, on the suspicion that the textbook was lagging the street — they were not reckless. They were paying attention.

Sources
Wang RC, et al. "Naloxone and Clinical Outcomes in Suspected Opioid-Associated Out-of-Hospital Cardiac Arrests." JAMA Network Open. 2026 (article 2849629).
Grunau B, Rea T. "Naloxone for Out-of-Hospital Cardiac Arrest Due to Opioid Toxicity" [editorial]. JAMA Network Open. 2026 (2849636).
Quinn E, et al. "Naloxone and Patient Outcomes in Out-of-Hospital Cardiac Arrests in California." JAMA Network Open. 2024 (2822449).
Lavonas EJ, et al. "2023 American Heart Association Focused Update on the Management of Patients With Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning." Circulation. 2023;148:e149–e184.
American Heart Association. "Opioid-Associated Out-of-Hospital Cardiac Arrest: Distinctive Clinical Features and Implications for Health Care and Public Responses" [Scientific Statement]. Circulation. 2020.
NaCRA (Naloxone for Opioid-Associated Out of Hospital Cardiac Arrest) — ClinicalTrials.gov NCT06251609.
NACARDI Decision Instrument for Targeted Antidotal Therapy in Occult Opioid Overdose Precipitated Cardiac Arrest. 2026.
UC Davis Health. "Naloxone use during cardiac arrest linked to improved survival" [press release]. May 2026.


Comments