
Intraosseous Access: Why Not?
- John Gomez

- May 24
- 12 min read
Why Intraosseous Access Is Still One of the Most Underused Tools in Emergency Care

The Case That Started This
A colleague sent me a single image last week.
A ZOLL monitor. Twelve-lead pulled up. HR 203. BP 85/54. RR 61. SpO2 94%.
The tracing was almost impossible to interpret because of artifact, but the vitals told the story before the rhythm strip ever could.
This was a patient minutes from crashing.
The eventual disposition matched the physiology: urinary tract infection, septic shock, and a patient standing on the edge of decompensation.
And here is the part that made me write this.
They could not get IV access in the arms or hands.
Two attempts. No access. A septic shock patient with a heart rate over 200, a respiratory rate over 60, a blood pressure in the tank, and a clock that was not slowing down for anyone.
So I will ask the question I have been asking for years:
Why didn’t anyone drill?
Intraosseous access remains one of the most underused interventions in emergency medicine. Not because it does not work. Not because the evidence is absent. Not because it is exotic, experimental, or reserved for some mythical last-ditch scenario.
In my opinion it is underused because of culture, training decay, discomfort, and a stubborn cognitive bias that still treats IO as a failure pathway instead of a parallel pathway.
This post is the case for changing that.
Not recklessly. Not theatrically. Not because drilling looks cool.
Because physiology does not care how many peripheral IV attempts we planned to make.
What the Guidelines Already Say About Intraosseous Access
Let’s start with what is already on paper.
Emergency nursing, resuscitation, trauma, and prehospital guidance all support IO access when vascular access is urgently needed and peripheral IV access is delayed, unsuccessful, or not feasible.
The Emergency Nurses Association and Infusion Nurses Society position is straightforward: trained clinicians may insert and manage IO devices, and IO access should be considered as a first alternative when peripheral access cannot be obtained or attempts fail in patients who medically require vascular access.
AHA resuscitation guidance continues to prefer IV access when it can be obtained quickly, particularly during cardiac arrest, but IO remains an accepted alternative when IV access is not feasible, delayed, or unsuccessful.
ATLS, ACLS, pediatric resuscitation guidance, and many EMS protocols reflect the same operational truth:
When the patient is unstable and vascular access matters, we should not burn the clock chasing peripheral veins indefinitely.
Many EMS systems operationalize this with a simple threshold:
Two unsuccessful peripheral IV attempts in an unstable patient should trigger serious consideration of IO access.
Some protocols are even more direct.
If the patient is unstable, needs medication or fluid replacement, and peripheral access is not rapidly available, IO is not a dramatic escalation.
It is appropriate vascular access.
The threshold exists. The recommendation exists. The equipment exists. The practice often lags behind all three.
IO Is Not a Compromise Route
The most persistent myth about IO access is that it is somehow “less than” vascular access.
A backup. A bridge. A consolation prize. Something we do after everything else fails.
That framing is wrong.
Intraosseous access places fluid and medication into the medullary cavity of bone, which functions as a non-collapsible venous plexus. From there, medications and fluids enter central circulation.
In shock states, that matters.
Peripheral veins collapse. Patients vasoconstrict. Dehydration worsens access. Sepsis alters vascular tone. Trauma patients clamp down. Pediatric patients disappear their veins completely. Obese patients may have veins that are impossible to identify quickly.
The bone does not collapse.
That is the point.
IO access is not a fake IV.
It is vascular access through a different door.
First-Attempt Success and Time Matter
In emergency care, access is not an academic exercise.
Access is time.
Time to fluids. Time to analgesia. Time to sedation. Time to antibiotics. Time to vasopressors. Time to resuscitation.
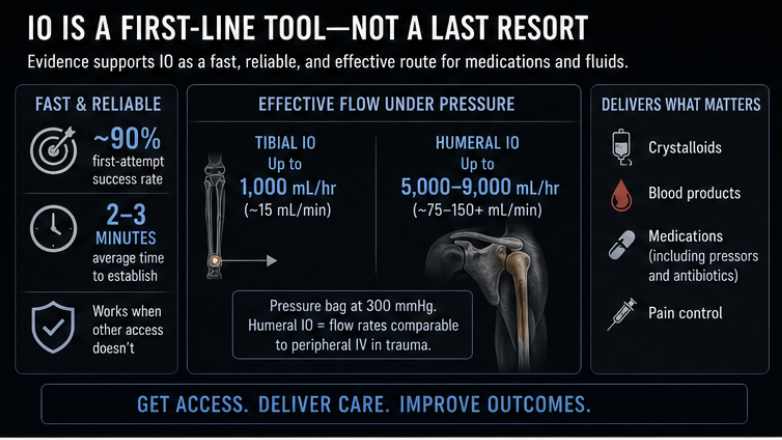
Multiple studies and reviews have found high first-attempt success rates with modern IO devices, often around 90% or higher depending on site, device, patient population, and operator experience.
That does not mean every IO attempt succeeds. It does not mean technique does not matter. It does not mean humeral placement is as easy as tibial placement in every patient.
But compared with repeated peripheral attempts in a crashing patient, IO is often faster, more reliable, and more physiologically honest.
The average difficult IV can consume several minutes. Sometimes many minutes. Sometimes it never happens.
In a stable patient, that may be acceptable.
In septic shock, status epilepticus, major trauma, profound hypoglycemia, peri-arrest respiratory failure, anaphylaxis, or severe hypotension, it may not be.
The question should not be:
“How many IV attempts do I get before IO?”
The better question is:
“How long can this patient afford to wait for access?”
Flow Rates: The “IO Is Just a Trickle” Myth
Another common myth is that IO access cannot support meaningful resuscitation.
That is only partly true — and usually because the IO is being used incorrectly.
Gravity flow through an IO is often poor.
That is expected.
The medullary cavity is not a big floppy peripheral vein. To achieve meaningful flow, IO infusion usually requires a pressure bag, push-pull technique, or infusion pump depending on the clinical situation and local protocol.
When pressurized appropriately, IO can deliver clinically useful flow rates.
The site matters.
The proximal tibia is common, familiar, and often technically straightforward. But the proximal humerus generally provides higher flow rates and faster transit to central circulation in adults when properly placed and secured.
That does not mean humeral is always better.
The humeral site can be more technically demanding. It can be easier to dislodge if the arm is moved. Landmarks can be harder in some patients. In cardiac arrest, ongoing CPR and patient movement may make tibial placement more practical.
But for the perfusing adult shock patient — especially one who needs rapid medication delivery, pressors, or substantial fluid movement — the proximal humerus deserves more attention than it often receives.
We should not default to tibial simply because that is where the manikin had the hole.
Septic Shock: The Patient Who Cannot Wait
The case that triggered this article was septic shock.
That matters.
Sepsis is a time-sensitive disease process. In septic shock, every delay in resuscitation can worsen organ dysfunction. Early recognition, early antibiotics, source control, hemodynamic support, and appropriate resuscitation all matter.
EMS does not usually administer antibiotics in most systems, although some services do under specific protocols. But EMS absolutely controls several critical early moves:
Recognizing possible sepsis
Supporting oxygenation and ventilation
Establishing access
Beginning fluid resuscitation when appropriate
Considering vasopressors where protocol allows
Trending perfusion and mental status
Communicating sepsis concern early
Reducing downstream delay
None of that happens efficiently without access.
A septic shock patient with failed peripheral IV attempts should not become a pin cushion while everyone waits for magic.
If the patient is unstable and access is needed now, IO should be in the front of the clinician’s mind — not buried under five more attempts and a prayer.
The patient does not care whether the access is peripheral IV, ultrasound-guided IV, central line, or IO.
The patient cares whether the resuscitation starts before compensation fails completely.
The Honest Reasons We Still Hesitate
If the evidence and guidelines support IO, why do we still underuse it?
In my experience, five reasons keep showing up.
1. Clinician Discomfort
Drilling into bone feels invasive.
It feels dramatic. It feels aggressive. It feels like something we should save for the absolute worst moment.
But let’s be honest.
Repeated failed peripheral IV attempts in a crashing patient are not benign.
They cause pain. They waste time. They delay treatment. They create stress. They may give the team the illusion of progress while the patient deteriorates.
The procedure that feels more invasive is not always the procedure that is more harmful.
2. The “I Can Get This IV” Trap
Most clinicians who are good at IVs know they are good at IVs.
That confidence is useful — until it is not.
There is a point where persistence becomes ego.
Attempt three.
Attempt four.
“Let me try one more.”
“Get the light.”
“Try the hand.”
“Try the thumb.”
“Maybe the EJ.”
Meanwhile, the patient is still hypotensive, still tachypneic, still altered, still crashing.
The clock does not care how good you usually are.
Two failed attempts in an unstable patient should trigger a change in strategy.
Not eventually. Now.
3. The Myth That IO Is Second-Class Access
IO is often treated as a placeholder until “real access” is obtained.
That mindset needs to die.
IO is temporary, yes. It should be replaced by more definitive access when practical. It requires monitoring. It has complications. It is not meant to live in the patient forever.
But during resuscitation, it is real access.
Many emergency medications and fluids can be administered through IO access when permitted by protocol and manufacturer guidance. This includes common resuscitation medications, crystalloid, blood products in many systems, sedatives, analgesics, anticonvulsants, and vasopressors.
The correct framing is not: “Can we get by with an IO?”
The correct framing is: “Does this IO allow us to begin the resuscitation this patient needs right now?”
Often, the answer is yes.
4. The Pain Myth
Awake IO patients can experience significant pain during infusion.
Not usually from the insertion itself.
From pressure inside the medullary space during flushing and infusion.
That pain is real.
But the conclusion should not be “IO is cruel.”
The conclusion should be “manage the pain correctly.”
Many protocols recommend preservative-free lidocaine through the IO hub before flushing or pressurized infusion in conscious patients who are not allergic and when not contraindicated. Dosing, concentration, dwell time, and repeat dosing vary by system and device guidance, so clinicians should follow local protocol.
Operationally, most systems administer lidocaine after confirming IO placement and before aggressive flushing or pressure infusion.
A common adult approach is:
Slow IV/IO push of preservative-free lidocaine through the IO
Allowing a short dwell time
Followed by a saline flush before infusion begins
Many systems use approximately 20–40 mg initially in adults, with repeat dosing permitted depending on patient response and protocol. Pediatric dosing is typically weight-based.
The important point is not memorizing a single universal dose.
The important point is understanding that infusion pain can often be reduced dramatically if clinicians proactively manage it instead of ignoring it.
If awake IO infusion hurts and the clinician skipped the lidocaine step, the problem is not the IO.
The problem is technique.
5. Training Decay
IO is a classic high-risk, low-frequency skill.
Most providers are trained on it. Few use it often. Some have never placed one on a live patient. Many have not touched the drill since initial training.
That creates hesitation.
Hesitation creates delay. Delay reinforces underuse. Underuse worsens skill decay.
The cycle continues.
If agencies want IO used appropriately, they cannot treat it as a once-a-year competency checkbox.
They need deliberate practice. Landmark refreshers. Scenario-based triggers. Pain-management rehearsal. Humeral and tibial site training. Securement practice. Complication recognition. And honest after-action review when access delays occur.
Humeral vs. Tibial: Choose Deliberately
The proximal tibia is familiar, easy to teach, and often reliable.
It is a good site.
But it should not be the only site clinicians think about.
The proximal humerus often provides advantages in adult perfusing patients:
Faster medication transit to central circulation
Higher achievable flow rates under pressure
Better option for larger-volume infusion compared with tibial in many studies
Potentially better pharmacokinetic profile for some emergency medications
But humeral IO is not magic.
It requires accurate landmarking. It requires proper arm positioning. It requires aggressive securement. It can dislodge if the arm is moved. It may be harder in obesity or difficult anatomy. It may not be ideal during chaotic CPR depending on the team and patient position.
So the point is not “humeral always.”
The point is “do not choose tibial by habit.”
Choose the site that best fits the patient, the resuscitation goal, the team’s skill, and the environment.
That is what professionals do.
Cardiac Arrest: Where the Evidence Is More Nuanced
This is where we need to be clinically honest.
IO access is clearly useful when IV access cannot be obtained quickly. But in adult out-of-hospital cardiac arrest, the evidence comparing IV and IO is more complicated than older teaching sometimes suggests.
AHA guidance generally favors IV access first when it can be obtained without delaying care. IO is appropriate when IV access is unsuccessful or not feasible.
Several observational studies have associated IO access with worse outcomes compared with IV in cardiac arrest. That does not prove IO causes worse outcomes, because IO may be used in harder, sicker, more chaotic cases where IV access was already difficult. But it does mean we should avoid pretending IO is automatically equivalent in every arrest scenario.
Some pharmacokinetic research suggests drug delivery through certain IO sites, particularly tibial IO, may produce slower peak central concentrations than IV administration.
That may matter when medication timing and peak concentration are important.
So here is the balanced operational takeaway:
If a skilled clinician can rapidly obtain IV access during cardiac arrest without delaying compressions, defibrillation, ventilation, or medication administration, IV remains preferred.
If IV access is delayed, unsuccessful, or unrealistic, IO is appropriate and should not be delayed.
Nuance matters.
But nuance should not become paralysis.
The Reframe That Changes Behavior
IO is not an escalation.
IO is a parallel pathway.
The decision tree should not be:
Peripheral IV → peripheral IV → peripheral IV → maybe EJ → maybe ultrasound → maybe IO → maybe central line.
The decision tree should be:
What is the fastest reliable route to circulation that supports the resuscitation this patient needs right now?
Sometimes that is a 20-gauge in the AC. Sometimes it is an ultrasound guided IV. Sometimes it is an EJ. Sometimes it is a humeral IO. Sometimes it is a tibial IO. Sometimes, later, it is a central line.
The route matters less than the mission.
The mission is timely resuscitation.

Back to the Case
A patient with suspected septic shock, HR 203, BP 85/54, RR 61, SpO2 94%, failed peripheral access, and impending decompensation is not a patient who should wait through endless access attempts.
That patient needs a change in strategy.
Two failed peripheral attempts should have triggered IO consideration immediately.
Not because IO is flashy. Not because the drill is fun. Not because every difficult IV requires IO.
Because this patient was unstable, access was needed, and delay had consequences.
That is the whole argument.
The Operational Takeaway
If you teach, train, supervise, or run an EMS agency, ED, urgent care, flight program, tactical team, or critical care transport service, three things would move the needle immediately.
1. Set the Threshold Clearly
Do not leave IO activation entirely to vibes.
Build a simple operational trigger:

For peri-arrest patients, profound shock, active seizure, critical hypoglycemia, severe trauma, or anaphylaxis, the threshold may need to be even lower depending on protocol and clinical context.
2. Train the Whole Procedure, Not Just the Drill
IO education should begin with reasoning — not the drill itself.
Too many providers are subconsciously taught: “Cardiac arrest equals IO.”
That framing is incomplete.
IO is not simply a cardiac arrest skill.
It is a vascular access strategy.
Providers should be trained to think about IO as a parallel pathway whenever critically ill patients need rapid access and peripheral access is delayed, difficult, or failing.
That means scenario training should include:
Septic shock
Major trauma
Status epilepticus
Severe dehydration
Profound hypoglycemia
Anaphylaxis
Respiratory failure
Burn patients
Difficult-access bariatric patients
Dialysis patients
Pediatric shock
Peri-arrest physiology
The goal is not to create providers who drill recklessly.
The goal is to create providers who recognize when continued IV attempts are actively harming the resuscitation timeline.
IO training should also include:
Site selection
Landmarking
Needle size selection
Confirmation
Flushing
Pain control for conscious patients
Lidocaine administration and timing
Pressure infusion
Securement
Ongoing assessment
Extravasation recognition
Complication management
Documentation
Transition to definitive access

If your IO training ends when the needle pops into the bone, your training is incomplete.
3. Stop Treating IO as Failure
This may be the most important culture shift.
IO is not what you do when you failed.
IO is what you do when the patient’s physiology demands faster access than the peripheral veins are willing to provide.
That is not failure.
That is clinical judgment.
Final Thought
The drill is one of the most powerful tools in emergency care.
Not because it is dramatic.
Because it turns delay into access.
And in emergency medicine, delay kills quietly.
The next time you are standing over an unstable patient with no IV, failed attempts, collapsing veins, worsening vitals, and a team still hoping the next stick will be the one, ask the question early:
Is it time to drill?
Because sometimes the most important intervention is not the medication, the fluid, or the pressor.
It is creating the route that lets those interventions arrive in time.
References and Further Reading
Emergency Nurses Association / Infusion Nurses Society. Position statements and guidance on intraosseous vascular access.
American Heart Association. Adult Advanced Life Support / ACLS guidance on IV and IO access.
International Liaison Committee on Resuscitation and AHA ECC guideline updates on IV vs IO access in cardiac arrest.
Montez D, Puga T, Miller LJ, et al. Intraosseous infusions from the proximal humerus reach the heart in less than 3 seconds in human volunteers. Annals of Emergency Medicine. 2015.
Dornhofer P, et al. Intraosseous Vascular Access. StatPearls / NCBI Bookshelf.
Paxton JH, Knuth TE, Klausner HA. Proximal humerus intraosseous infusion literature and emergency access reviews.
El-Nawawy AA, Omar OM, Khalil M. Intraosseous versus intravenous access in pediatric septic shock patients admitted to Alexandria University Pediatric Intensive Care Unit. Journal of Tropical Pediatrics. 2018.
Reviews and EMS protocol guidance on IO use in shock, resuscitation, and difficult vascular access.
John Gomez is the founder of and Black Flag EMS. He writes and teaches on high-risk, low-frequency emergency medicine, tactical medicine, tactical performance, physiology-driven clinical decision-making, and operational performance under stress.
#Paramedic, #EMS, #Healthcare, #IO, #IV



Comments